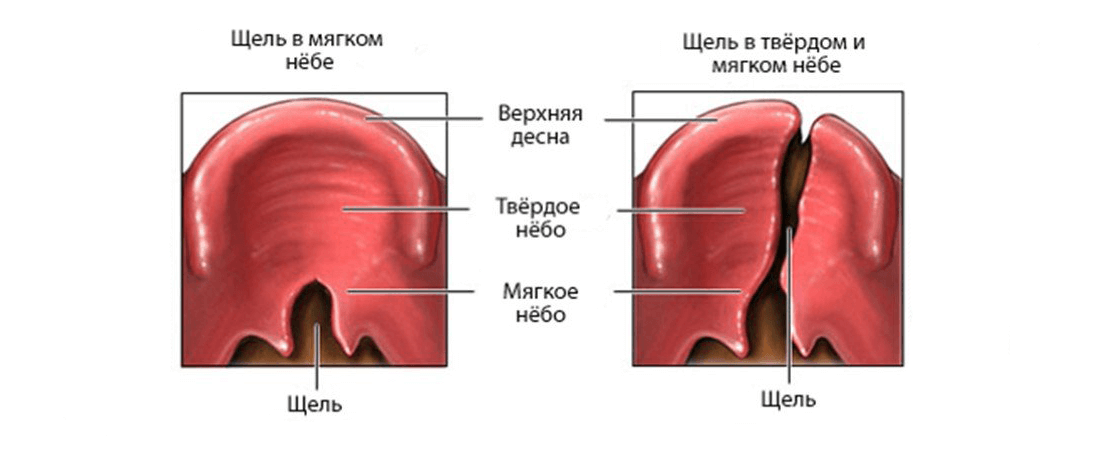
Wolf’s mouth or cleft palate
The embryonic development of the palate occurs between the 4th and 12th to 13th weeks of life. During this time, the basic morphology of the face is formed with the fusion of five main facial protrusions: along the midline, a frontal protrusion and a paired maxillofacial protrusion (Afshar, 2012).
The medial part of the frontal protrusion generates the primary palate, while the maxillary protrusions form the secondary palate. Each protrusion of the face consists of neural crest cells, which are ectodermal cells on the margins of nerve folds on a bilateral basis and a transitional area between the neuroectoderm and the epidermis, in segmental positions along the neural tube (Afshar, 2012).
Neural migration of crest cells into craniofacial and pharyngeal complexes is predetermined by inductive processes. Deficiencies in the migration or proliferation of neural crest cells are the source of a diverse range of cranial malformations, including cleft palate (Hall, 1999; Eppley et al., 2005). The separation of the oral cavity and nose occurs when the frontal nasal process and maxillary processes merge; fusion requires coordinated growth between the processes and epithelial apoptosis, which forms a transitional nasal bridge (fin) between paired processes (Mangold, 2011).
Cleft most often occurs between the primary and secondary palate, and initial mesenchymal deficiency, decreased premaxilla volume, increased apoptosis, or increased bone resorption due to lack of functional forces in the primary palate have been identified as causes of cleft (Siegel, 1985, 1991; Mooney et al., 1992).
Secondary fusion occurs from the anterior to the posterior margin, starting and ending with the fusion of the uvula of the soft palate (Smith, 2012).
Starting from the 8th week, the palatine plates rise from the vertical position surrounding the tongue to the horizontal position (Sperber, 2002b).
This movement is slightly delayed in women (Burdi and Faist, 1967).
After rotation, sutures are fused along the medial edges, and epithelial apoptosis is crucial for the normal secondary formation of the palate (Sperber, 2002b).
As the secondary palate closes, the mandibular protrusion grows and the tongue pushes forward into the oral cavity (Diewert and Lozanoff, 2002). Cleft palate can occur due to the inability of the palatine plates to rise and connect, which may be due to genetic, mechanical, or teratogenic factors that disrupt the processes of rotation and fusion of these protrusions (Afshar, 2012).
The severity of the cleft depends on the period of fetal development during which the disorder occurred (Friedman, 2010). The primary fusion of the sky usually ends between weeks 4-8, while the secondary begins to form during the 8th week, with completion around the 12th (Marazita and Mooney, 2004; Aalst, 2008).
In addition, the palate in women is known to close one week later than in men, increasing the risk of cleft formation, and confirms the current hypothesis of a higher incidence of cleft palate in women. Burdi and Silvey demonstrated this by finding that the critical week of palate closure will be the seventh for men and the eighth for women (Burdi and Silvey, 1969; Aalst, 2008).